
Menopause, Hormone Therapy, and the Brain
Menopause, Hormone Therapy, and the Brain
A deep dive into the 2024 Menopause Society Meeting

There was a fantastic session at the 2024 Menopause Society meeting on menopause and brain health. Four speakers covered cognition, dementia, and depression. Here, I am going to review my takeaways from the lecture on cognition, dementia, and Alzheimer’s disease, which was presented by Dr. Pauline Maki, PhD, and Jacob van Doorn, MS. I took extensive notes, but I have since re-listened (twice) to a recording of the session to cross-check and I also pulled some of the references that were quoted. It really was a fantastic lecture.
I know many people have heard from some corners of social media that estrogen therapy is VITAL for brain health (in caps to help get the faux urgency of these social media posts across), but I think after reading this you will feel a lot less panic and maybe a little anger about that messaging. I know some of these meno-influencers bemoan the lack of data in women’s health, but it’s rather hypocritical to do that and then ignore or mangle the science that we do have to promote a message that is interpreted by many as “every woman must take estrogen urgently now for brain health.” There are plenty of good reasons to prescribe hormone therapy, and lots of excellent researchers working to understand more about menopause, hormone therapy, and the brain, so we should let this research unfold! Isn’t that what we want? High quality research? I spoke to some amazing scientists working to answer the questions that we all have, which filled me with a lot of hope.
This is a long post, so if you just want the takeaways, head to the “Conclusions” section at the end! I’ve also included some of the relevant slides.
The 2022 Menopause Society Guidelines Hold: Menopause Hormone Therapy is NOT Indicated For Cognition or to Prevent Dementia
This was stated quite emphatically at the beginning and again towards the end of the talk. Dr. Maki was clear that people going against the guidelines…meaning those telling women that estrogen therapy is essential to prevent dementia…are operating in what she called a “data free zone.” In addition, she mentioned that shared decision making must be based on “rational evidence based scientific literature that is reliable and reproducible.” I bring this up, because shared decision making is health care professionals collaborating with their patients on evidence based treatment decisions, it’s not a “get out of jail free” card to offer non evidence based care.
The one caveat to in the brain health discussion, which was addressed in the lecture, is premature menopause (before age 45) and surgical menopause before age 48. In these situations menopause hormone therapy is the standard of care when safe to reduce the risk of dementia. For these women hormones are recommended until the average age of menopause, age 51-52, and then at that point a decision can be made about continuing for the standard indications.
What are the Cognitive Changes in the Menopause Transition/Menopause?
According to the American Psychological Association, “Cognition includes all forms of knowing and awareness, such as perceiving, conceiving, remembering, reasoning, judging, imagining, and problem solving.”
There is a lot of discussion about cognitive symptoms in the menopause transition and menopause (after the final period), but we must remember that are two variables here. Menopause is occurring, and we are also aging at the same time. This means studies are essential to distinguish between effects that could be due to menopause, and those that could be because we are getting older (as in even my husband misplaces his phone and keys all the time and he is definitely not going through menopause). It’s also essential that we have longitudinal studies, where people are followed over time and both age and accurate stage of menopause are taken into consideration. And of course symptoms must be considered as well as medical conditions that could affect cognition.
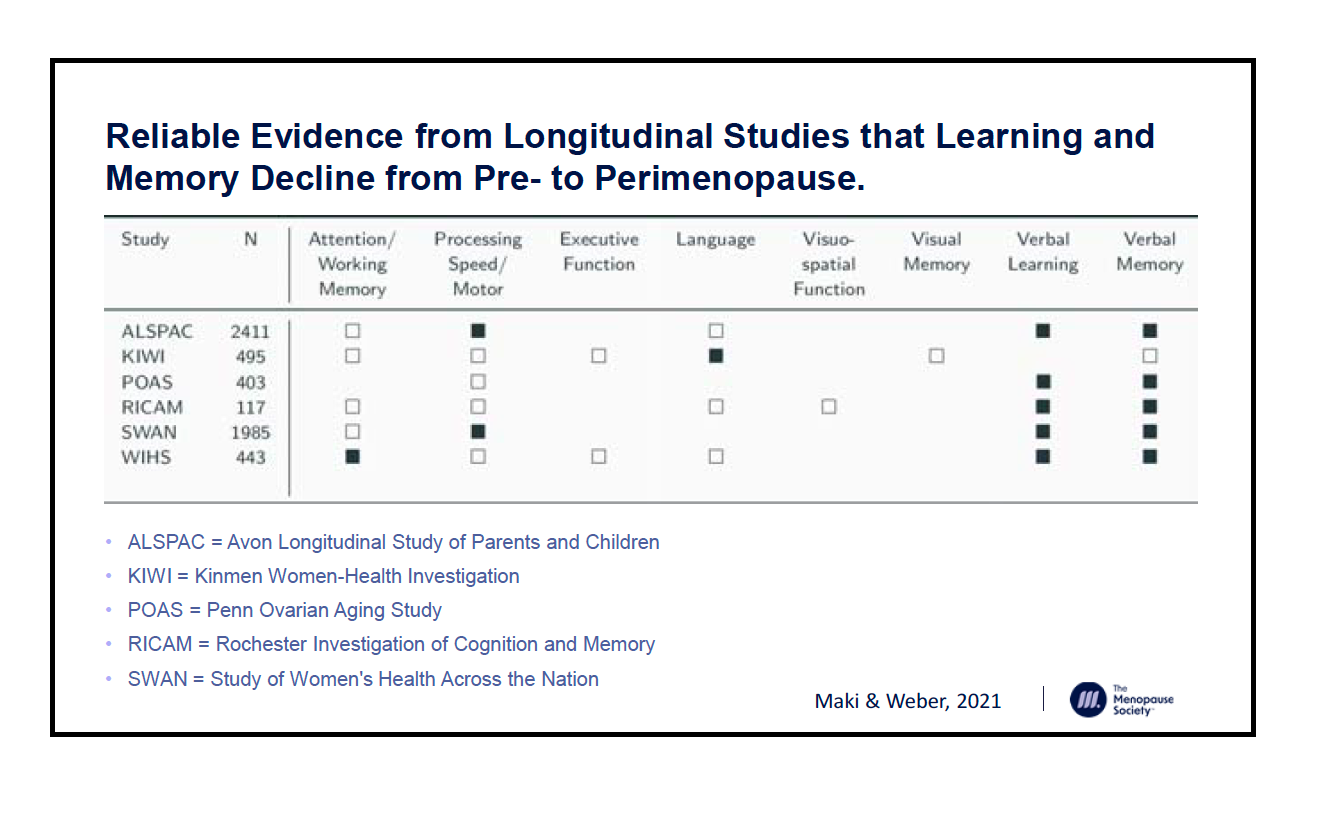
I know that many aspects of menopause are understudied, but there are at least six longitudinal studies that have evaluated cognitive changes, and two changes emerge as being consistently related to the menopause transition/early menopause: verbal learning and verbal memory. It’s also important to know that for most women these changes are reversible. Here is the slide that lists those studies, as well as the numbers of participants
There is a notable gap in the literature when it comes to ADHD, and there are some cross sectional studies that suggest a higher rate of ADHD like symptoms in the menopause transition and early menopause. Estrogen is involved in executive function, so there is a plausible connection here. There has been some work looking at the use of stimulant medications for ADHD for women experiencing these symptoms. However, there is a big asterisk here as a worsening or development of ADHD like symptoms and treatment with stimulants have not been evaluated over longitudinal studies.
Menopause Hormone Therapy and Cognition: Baseline Information
As there are some cognitive changes in the menopause transition, might they respond to menopause hormone therapy?
There are four randomized double blinded placebo controlled trials looking at MHT for cognition, and these studies have looked at different hormone regimens,