


Correcting Disinformation about Depo-Provera
It's a quagmire on Instagram


I’ve been tagged many times in a Depo-Provera infographic making the Insta rounds. The title is “What I wished I’d known about Depo-Provera”, which insinuates that medical professionals are keeping this vital information from you. As most of the information presented in the infographic is incorrect or misleading, no doctor or nurse practitioner should actually be warning you about these points!
Whether this infographic comes from a person who feels they have been harmed by Depo-Provera, so in good faith but incorrect nevertheless, or an anti-birth control warrior, so in bad faith, I don’t know. As an aside, anti birth control warriors are either naturopath/functional medicine types or someone who wants to impose their religion on others, and I find the overlap between these two groups fascinating. I regularly get insulted by accounts that can be best described as either “natural loving mama” and ‘Jesus loving mama”, and when I look at them they appear identical.
Regardless of the source, it is important to state that many people don’t receive adequate counseling about contraception, but the response should not be a campaign of misinformation and disinformation. Rather, it is to demand that medicine and medical professionals do a better job and provide correct information, which is what I am about to do!
Before we begin. What is Depo-Provera?
Depo-Provera is the trade name for an injectable medication called depot medroxyprogesterone acetate, commonly abbreviated as DMPA. Depo-Provera or DMPA is a progestin, meaning it is a hormone made in a lab that is similar in many ways to the hormone progesterone. While it is most commonly used as a hormonal contraceptive, it is also used for management of endometriosis and bleeding from fibroids.
Depo-Provera has benefits and it has side effects and it has risks…like every medication. And a good practitioner reviews these with their patient before the medication is started. This is one of the tenants of informed consent, because you can’t make an informed decision with incorrect information. In addition, people are more satisfied with their method of contraception when they are fully informed.
The main benefit of Depo Provera is that it is one of the most effective methods of contraception, the failure rate for those who get their injection on time is 0.3%. In addition, there is no need to remember to take something daily or to use contraception during sex, which is very important to many people. It is also reversible.
Irregular bleeding is a common side-effect when Depo-Provera is first started. This should be discussed in detail before beginning, because if a person doesn’t think they can handle what could be (not always, but could be) irregular bleeding for at least 3 months and possibly longer, then this may not be the right method for them. The bleeding with Depo-Provera is typically lighter than a period, and so the trade off is a reduction in the amount of blood lost, and this may even help reverse iron deficiency anemia.
Over time the bleeding with Depo-Provera decreases. By the end of one year of use, 50% of people will have no periods and by two years that number rises to 68%. There are some strategies for treating irregular bleeding on Depo-Provera for people who are in the percentage with persistent issues. Someone with regular, light periods might find the potential for irregular bleeding unacceptable and someone whose period is 8 days of flooding might find the trade off for irregular spotting absolutely worth it. For some, a 68% chance of having no periods after two years with the potential of having to deal with irregular bleeding in the interim, is a perfectly acceptable trade-off. For others, it is not. This is why good contraceptive counseling matters
Depo-provera also reduces pain with periods.
Because Depo-Provera suppresses ovulation, it is an excellent choice for those who are on blood thinners and get bleeding into their ovaries with ovulation (hemorrhagic corpus luteum). It also reduces: the risk of cancer of the endometrium (uterine lining) by 80%, the risk of ectopic pregnancy, and sickle-cell crises for women with sickle cell disease.
Another benefit of Depo-Provera is the lack of estrogen, so many people who can’t safely take estrogen-containing birth control pills can safely use Depo-Provera. The lack of estrogen also makes Depo-Provera a good contraception option for trans men who need contraception.
The downsides of Depo-Provera includes the irregular bleeding as just discussed. There is also an impact on bone density, which will be discussed below along with some other risks shortly. There is some data suggesting that Depo-Provera may increase the risk of acquiring HIV if exposed, but this is unclear.
Another very important part of the benefit-risk discussion is how important it is for the person to not get pregnant. Someone who absolutely must not get pregnant may view side effects like irregular bleeding differently from someone who is less concerned about a contraceptive failure. Another consideration is abortion availability and cost for those who would or might choose abortion should they have a contraceptive failure. For example, an unplanned pregnancy in Texas may have different ramifications than an unplanned pregnancy in California based on access to abortion.
Okay, let’s get started. Here’s the infographic

CLAIM: Depo provera is used to chemically castrate sex offenders — eliminating or severely reducing sex drive.
This scenario does not apply to someone with ovaries. Hormonally speaking, the brain-testicles connection is not the same as the brain-ovary connection. This argument shows how disingenuous the person or people behind this infographic actually are. Medications used for anesthesia are also used for executions, but that doesn’t make these medications bad because a general anesthetic isn’t an execution. Leading with an entirely unrelated subject means you have no argument. You should be opening with your strongest argument, not what would be a major gaffe for a middle school debate.
There are many ethical issues with chemical castration for sex offenders with testicles, but none of those apply here because we are talking about ovaries. Testicles and ovaries are different organs. I should not have to spell that out.
What about the impact of Depo-Provera on sex-drive for people with ovaries? In clinical trials that enrolled over 3900 women, six percent had a decrease in libido. So is it possible? Yes. Is it common? No. However, the fact that 94% of people experience no negative impact on libido is not exactly a strong argument against its use, so you can see why the people/person behind this infographic had to change the topic to the testicles.
CLAIM: It now carries the FDA’s strongest black-box warning because it can cause significant bone density loss and increase the risk of osteoporosis.
There are no degrees of black box warning, this isn’t Karate. There is no progression in black box warning colors to the pinnacle of black box. There is a black box warning or there is not. Many medications have black box warnings and these warnings don’t mean the medication is bad or good, what they mean is a risk has been identified, this risk may be real or theoretical, and the FDA feels a highlighted warning is indicated so it can be part of informed consent. A black box warning doesn’t mean a drug is too dangerous to use, it simply means pay attention.
It is important to point out that there are some issues with the FDA’s black box warning system, and this warning may exist when there is literally no risk. For example, vaginal estrogen has a black box warning and that is ridiculous as no credible study raises concerns.
Let’s get right to the disinformation before we even talk about the bones.
The black box warning does not state that Depo-Provera can “increase the risk of osteoporosis”, it says it is unknown. The “may not be completely reversible” is exactly that, “may not.” The risk regarding osteoporosis is described as “unknown.” You can read it here for yourself.

Admittedly, this warning could come off as scary, but the effects on bone density are not entirely clear. The bulk of the quality studies tell us the maximum reduction in bone density is about 5% and that for most people it is reversible. Breastfeeding is associated with a 3-5% decrease in bone density (also reversible), but no one is insisting breast-feeding have a black box warning.
There are issues with some of the studies on bone density. For example, women who choose Depo-Provera are also more likely to smoke and drink alcohol, and both are risk factors for low bone density. What we do know is the impact on bone density appears to be fully reversible for those who are under the age of 45.
ACOG (American College of Obstetricians and Gynecologists), the CDC (Centers for Disease Control and Prevention), SAHM (Society for Adolescent Health and Medicine), WHO (World Health Organization), and SOGC (Society of Obstetricians and Gynecologists of Canada) all believe the data shows that the benefits of of DMPA outweigh the bone density risks for most people and do not support the two-year limit. Loss of bone density appears reversible for everyone, with the exception of some adolescents who use Depo-Provera for more than two years, but there isn’t data to tell us if this is meaningful health-wise. Meaning we don’t know if for this group of teems more than two years of Depo-provera confers an increased risk of osteoporosis later in life or not. However, there is no good data supporting an increased risk of fractures.
The World Health Organization says there should be no restriction in use of Depo-Provera concerning bone density for those ages 18-45. For those younger than 18 and older than 45 the benefits typically outweigh the risks, but obviously individual counseling is required.
For example a 48 year old who smokes, or someone with limited mobility (lack of weight bearing increases the risk if osteoporosis), or a 16 year old with anorexia are all at higher risk of osteoporosis, so the potential impact of Depo-Provera on bone density requires a more in depth discussion. However, if that 48 year old needs Depo-Provera for contraception, their medical risks are much lower with Depo-Provera than with pregnancy. What if the person with limited mobility is using Depo-Provera for both contraception and to control very heavy periods and is avoiding a hysterectomy, which is a major surgical procedure, because of Depo-Provera? Context and individual benefit to risk discussions are needed. Translating this nuance to a blanket statement is either ignorance of malevolence depending on the motivation.
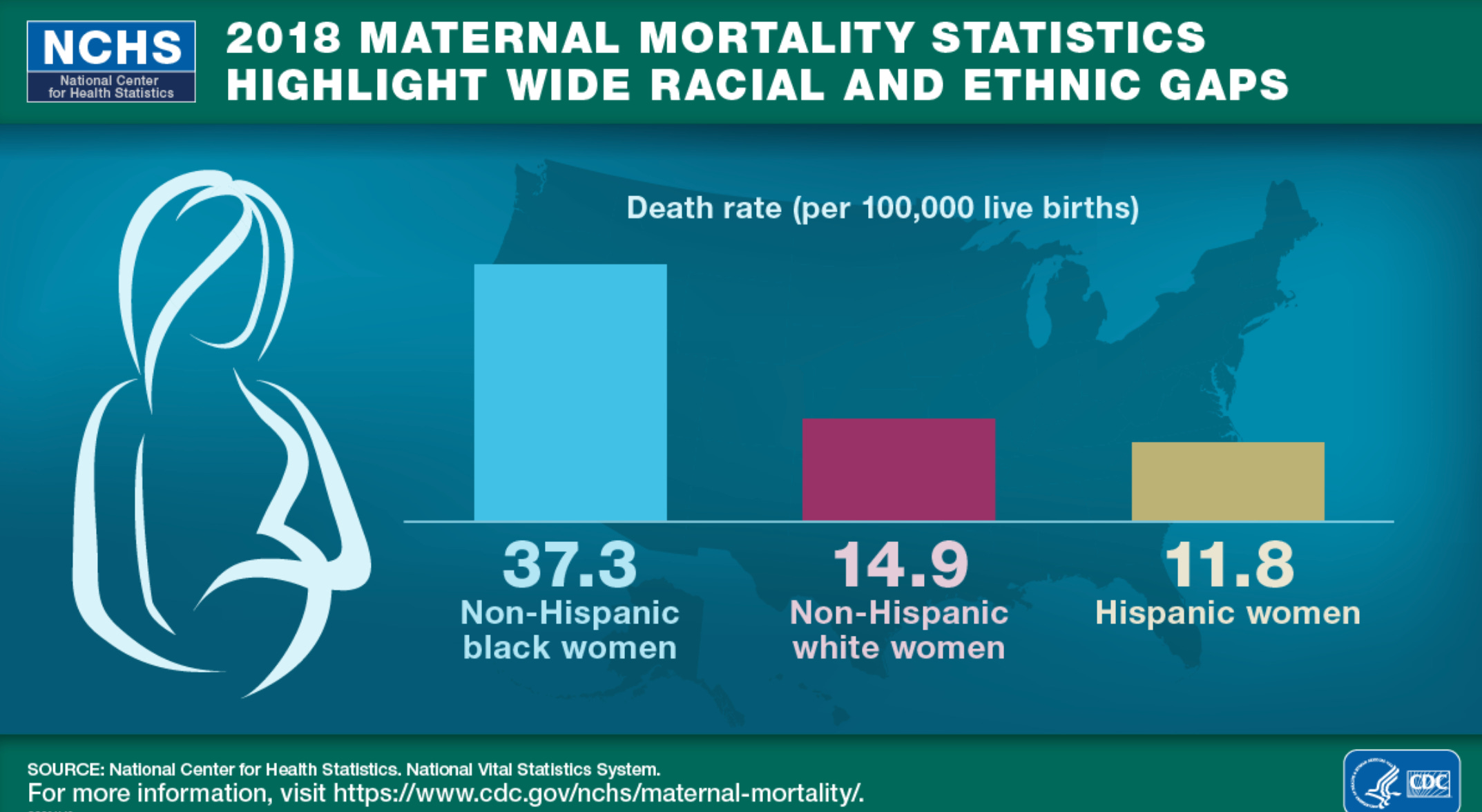
While we are discussing risks, you know what else should have a black box warning? Pregnancy! Pregnancy presents a risk of a potential fatal blood clot in the postpartum period (three months after birth) of 40-65/10,000 live births. Maternal mortality in the United States is 17.4/100,000 live births for all women and an even more shocking 37.3/100,000 live births for Black Women. Those opposed to certain contraceptives or who generate fear about contraception always seem to leave out these risks. We must be doing much more to reduce maternal mortality, especially for Black women, but contraceptive fear mongering isn’t part of any solution.
Claim: Unlike the weight gain from birth control pills that affect body weight primarily through fluid retention, Depo-Provera can change body composition and increase fat mass.
Studying weight and contraception is hard as the regular use of ALL contraception is associated with weight gain over time. We know this because the copper IUD is used as a control in many studies and that is method is associated with weight gain. Researchers don’t know if the need for contraception is associated with lifestyle changes that lead to weight gain or if this is a reflection of general weight gain with aging.
Unsurprisingly, studies on weight gain with Depo-Provera are all over the place, and so the best we can say is the data is conflicting, which is a lot less certain that the bold claim above. A detailed review on the subject from 2016 came to these conclusions:
The studies that compared Depo-Provera with the birth control pill showed no significant difference in weight gain.
Compared with non hormonal methods, one study showed an increase in fat mass of 11% for adolescents using Depo-Provera, however, another study looking at contraception after delivery showed no difference comparing Depo-Provera with a postpartum tubal ligation (a non hormonal method).
Several studies compared Depo-Provera with a copper IUD and found varying outcomes. The best quality studies (prospective) ranged from no difference to an increase in fat mass for those who used Depo-provera.
Is it possible that some people who use Depo-Provera may gain more fat mass than with other methods? Yes, but the data is not clear about this. One review of the data suggested that women who gain weight in the first 6 months on Depo-Provera may be the group at greatest risk for continued weight gain.
So weight gain something to look out for? Yes. Is this something that will definitely happen? No.
Claim: Other side effects include: nausea, uneven/persistent periods, depression, nervousness, hot flashes, migraines, fatigue, nightmares and dizziness.
The most complete data on side effects comes from two clinical trials with over 3,900 women who used Depo-Provera and who were followed for up to seven years. As there was no placebo arm, we don’t know if these side effects are due to the drug, are nocebo (negative placebo) effect, or due to something else. What this data tells us is as follows:
Nausea: 3.3% of users
Irregular bleeding: We addressed this above. It is common and requires counseling.
Depression: 1.5% of users It is possible that progestins could exacerbate depression for some, specifically those with PMS (premenstrual syndrome). A history of depression is not a contraindication against starting Depo-Provera. Women who may be at higher risk should have closer follow up after Depo-Provera is started. Pregnancy can also lead to depression, something always neglected in this aspect of the risk discussion.
Nervousness: 10.8% of users.
Hot flashes: 1 % of users.
Migraines: About 17% of people report headache, but headache or migraines is not a contraindication to starting. May trigger migraines for some. I do wonder about the data as people with migraines may be over represented among those who take Depo-Provera as some people with migraines can’t use estrogen containing contraceptives.
Fatigue: 4.2% of users.
Nightmares: I can find no studies backing up this claim.
Dizziness: 6% of users.
Claim: It can take up to 18 months for all the hormones to leave your body and may lead to infertility for up to two years after your last injection.
The delay in return to fertility after Depo-Provera is not infertility, it is an expected delay in return to fertility. I despise this abuse of the language. Using the word infertility here incorrectly is a deliberate attempt to stoke fear.
The latest data published in the British Medical Journal tells us the average time to return to fertility after Depo-Provera is 5-8 cycles. Assuming 28 days per cycle, that is 140- 224 days. Levels of Depo-Provera are undetectable by 120-200 days post injection, which fits with the typical delay in return to fertility.
Another study from the United States showed that the average time to getting pregnant is 10 months after the last injection, which is 7 cycles after the Depo-Provera has been stopped. This is in line with the study referenced above. In this American study, 68% of women were pregnant by 12 months after discontinuing Depo-provera. Keep in mind that over any one year period 85% of people trying to get pregnant actually get pregnant. So it is important to compare the 68% post-Depo-provera pregnancy rate at one year to 85% and not to 100%. By 15 months, 83% of people who have discontinued Depo Provera can expect to be pregnant and 93% by 18 months from the last injection.
After stopping any method of birth control, if you are under the age of 35, you can expect that it may take up to 12 months to get pregnant and if you use Depo-provera that extends to 18 months. For those aged 35 or older, any delay may be less acceptable or it may be just fine, but again, that is part of the counseling conversation.
Okay, that was a deep dive into Depo-Provera.
What can we learn from this? People should definitely not be using the infographic we just dissected to make decisions about whether Depo-Provera is a good contraceptive option for them! Also, I’d be suspect of any accounts sharing this infographic. And finally, there is a lot of fear mongering regarding Depo-provera. Basically, it gets blamed for everything.
Contraception is very personal, and the best way to help someone decide the best method for them is to give them all the information in an unbiased way.
And if you like this post, I really think you will love my next book! I’ll let you know the title as soon as I can.
Selected References
Yland JJ, Bresnick KA, Hatch EE, et al. Pregravid contraceptive use and fecundability: prospective cohort study. BMJ 2020; 371
Product monograph, Depo-Provera https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/020246s036lbl.pdf
https://www.cdc.gov/nchs/maternal-mortality/index.htm
guttmacher.org https://www.guttmacher.org/fact-sheet/contraceptive-use-united-states
Depot medroxyprogesterone acetate and bone effects. Committee Opinion No. 602. American College of Obstetricians and Gynecologists. Obstet Gynecol 2014;123:1398–402.
Depo medroxyprogesterone acetate (DMPA): Efficacy, side effects, metabolic impact, and benefits. UptoDate. AM Kaunitz.