

"I've Started Vaginal Estrogen, and I Still Have Bothersome Symptoms"
3 Steps to Figure Out Why

Vaginal and vulvar changes of menopause, known as genitourinary syndrome of menopause or GSM, affect up to 80% of women. For some, the symptoms start after their final period, but for others, they can start before the last period (in the menopause transition). While vaginal estrogen is highly effective, some women start this therapy yet still have symptoms.
How to proceed?
Before we go any further, I want to briefly discuss what happened to Halle Berry–her vaginal symptoms of menopause were misdiagnosed as herpes. While this is an extreme example of misdiagnosis, it doesn’t surprise me. I often see people with GSM who have been misdiagnosed with other conditions. Sometimes, what I can only call wildly misdiagnosed. This is one of the reasons that I do what I do. When you have the knowledge, you know if you are getting good care or not. As you read further and we discuss some of the conditions that might mimic GSM, you will see that herpes is nowhere to be found. This is because I can’t conceive of a scenario where GSM could be misdiagnosed as herpes. I really can’t. Herpes causes outbreaks, typically intensely painful symptoms (blisters and then ulcers) that resolve within 1-2 weeks without treatment, a little faster with antiviral medication (the first outbreak possibly a little longer). Genitourinary syndrome of menopause doesn’t go away without treatment (with estrogen, it will take 4-6 weeks to improve!). A herpes outbreak is also localized, meaning the pain, blister(s), and ulcer(s) will be in one spot. In contrast, GSM is not localized. While herpes can sometimes involve the cervix and cause some pretty dramatic inflammation in the vagina, these changes shouldn’t be mistaken for GSM. When herpes of the cervix is suspected, a vaginal PCR test can easily confirm the diagnosis as soon as the lab can turn the test around (typically within 1-2 days).
Experiences like Ms. Berry’s, which reflect a lack of understanding on the part of the provider about both herpes and menopause, are why I write The Vajenda and why I wrote The Vagina Bible, and The Menopause Manifesto. My ideal world would be fixing all the issues that result in this kind of misdiagnosis. Still, until that happens, I can at least educate my readers so they know when they are getting good care, when they are not, and how to advocate for what they need.
What and Where Are the Symptoms?
When someone is referred to see me for persistent discomfort after treatment for GSM, the first thing I do is review the symptoms to make sure I understand exactly what my patient means.
I consider three main categories of symptoms:
Irritative symptoms: These can include itch, irritation, dryness, a sandpaper-like feeling, or other bothersome irritation. If there is vulvar itching, is it bad enough that you scratch or really, really want to scratch?
Pain symptoms: For example, pain with sitting, pain with bike riding, pain with sexual activity, and pain all the time or that is intermittent and comes and goes.
Vaginal discharge: This can be bothersome in terms of amount, color, or odor.
Sometimes, people can’t decide between irritative symptoms and pain, and that’s okay. And, of course, people can have both irritative symptoms and pain.
I also typically think of four locations of symptoms:
Inside the vagina: As in reaching inside to find a tampon. In the image below, that corresponds to inside the black line at the vaginal opening.
The vestibule: The tissue that forms the boundary between the vagina and the vulva.
The vulva: The labia minora outwards. A good way to think of the vulva is where clothes touch the skin.
Around the anus: It’s important to clarify as often the anus gets lumped in with the vulva.
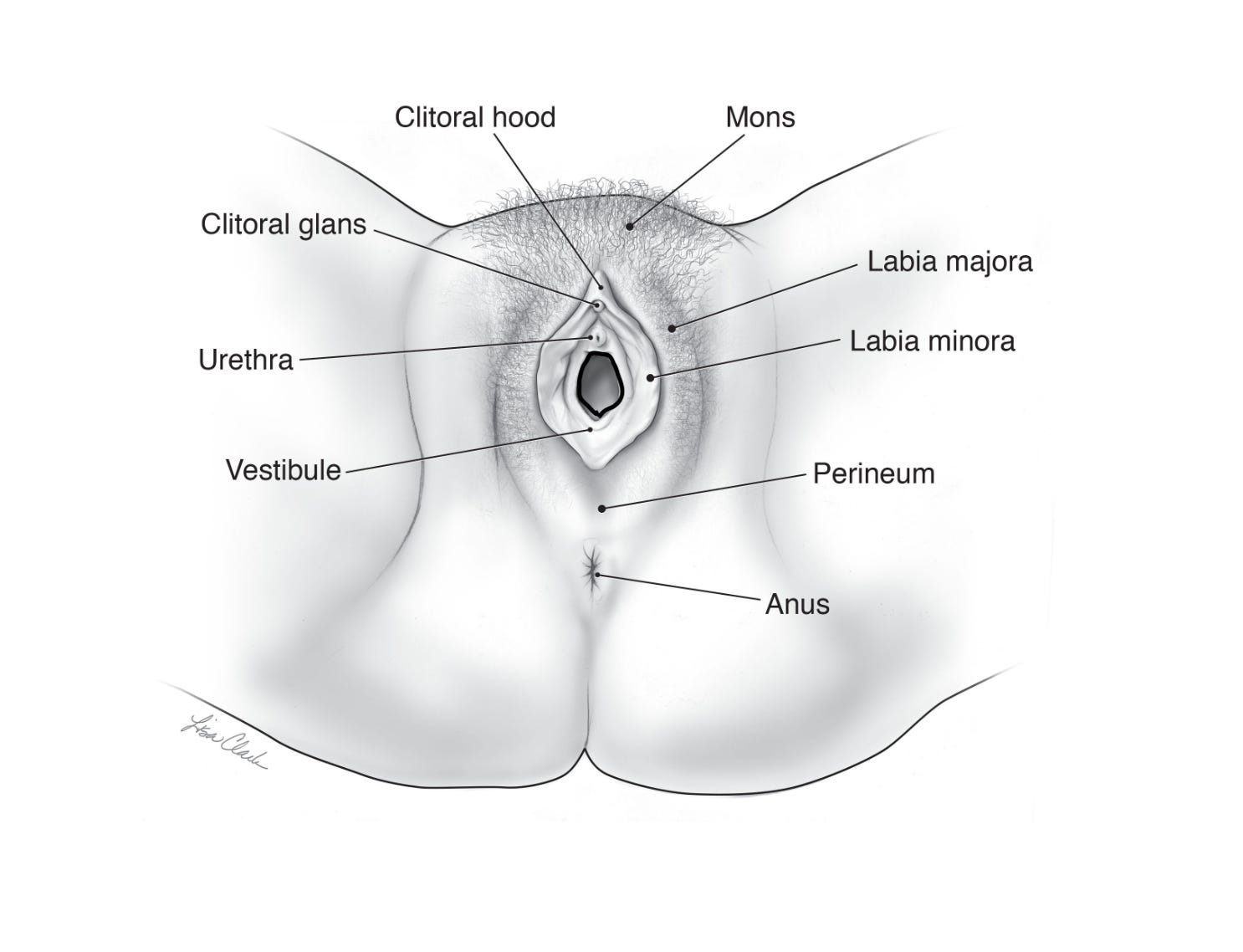
Considering what exactly is bothersome and the location can help narrow down the causes. For example, vulvar itching that is bad enough to scratch is typically a vulvar yeast infection or lichen simplex chronicus (see below). Knowing the bother factor and location is also an excellent way to communicate with your provider about your symptoms. For example, you might say:
I have itching at my vaginal opening and on my inner labia.
Or
I have a yellowish vaginal discharge, irritation at the vaginal opening, as well as pain, and a sand-paper-like feeling with intercourse. (This is a classic textbook description of GSM).
You can even use the image above to communicate with your provider.
The Causes of Vulvar and Vaginal Symptoms
Broadly speaking, there are two different reasons that symptoms might not resolve with vaginal estrogen (and sometimes both can be in play). The first is that GSM hasn’t been treated adequately. This is more likely to be the case when someone is using the lower doses of vaginal estrogen, either the 4 or 10-mcg vaginal inserts or 10-mcg tablets (read more about dosing here). It’s also possible that the inserts and tablets are treating the vagina, but they aren't delivering enough estrogen to the vestibule.
Symptoms of GSM include vaginal discharge, vaginal odor, vaginal or vestibular irritation and/or pain, pain with sex, vaginal dryness, a sandpaper-like feeling, pain with urinating, a feeling of razor-blades with sex, and pain with sitting. On exam, there may be little red dots at the vestibule and in the vagina, which are broken blood vessels known as punctate hemorrhages, and they are typical of GSM. Sometimes the vagina and/or vestibule appear red, but other times they can be pale. The vestibule and vagina might be very tender when touched with a Q-tip, and the vaginal pH is typically elevated (5.0 or greater). A vaginal sample should show inflammation (the very small darkish cells or dots in the photo below), and the epithelial (skin) cells of the vagina become small and round (the arrow is pointing to one). The type of estrogen regimen, the exam, the vaginal pH, and how the discharge looks under the microscope can all help us make a diagnosis of inadequately treated GSM.

The other possibility is that something other than GSM is causing symptoms. For example, GSM can cause vaginal dryness, but so can a yeast infection, and GSM can cause itching in the vagina or at the vestibule, but so can yeast, contact dermatitis, and some skin conditions. Here are the most common diagnoses to consider when GSM has been adequately treated based on the physical exam, yet symptoms persist:
Keep reading with a 7-day free trial
Subscribe to The Vajenda to keep reading this post and get 7 days of free access to the full post archives.