


Liver Disease and Menopause Hormone Therapy
Understanding the contraindications


Not every person can safely take every medication, and hormone therapy is no exception. Although, unlike many other medications, the list of conditions that make the estrogen and progesterone/progestins in menopausal hormone therapy (MHT) not the safest choice is actually relatively short.
We’ve already addressed the importance of age and time since the last period in starting MHT and the risk of clots. (For the full Table of Contents for what has already been covered in the Hormone Menoverse Series and what’s to come, click here). For this next post, I’m going to address one of three remaining big medical conditions that should be considered before starting MHT: liver disease.
Some Basics
Liver disease is more common than people think; it affects more than 10% of adults in the United States. It’s a fairly broad category, so there are a lot of different conditions included in the umbrella term “liver disease.” Many people think of alcohol when they consider liver disease; to be sure, it is an important cause (and sadly, a rapidly rising cause of death for people in their 20s and 30s). Still, those who don’t drink should also be mindful of their liver because there are many conditions that can have serious consequences for the liver, and one condition, nonalcoholic fatty liver disease (NAFLD), is especially of concern for women in the menopause transition and menopause, so much so that I will be addressing this in future posts.
When considering MHT, it’s important to think about the liver as this is where the hormones are metabolized, meaning they are repackaged and sent out into the blood or converted into other hormones before being packed up and sent off to work for the body. We have to know if the liver is healthy enough to handle metabolizing hormones and also if the hormones could have a negative effect on the liver. Also, liver disease doesn’t happen in an organ silo; people with liver disease may have more risk factors for heart disease or blood clots or have other medical conditions that need to be considered MHT-wise. Your own medical team will be important in determining the possible risks for anyone with liver disease who wants to consider hormone therapy in menopause.
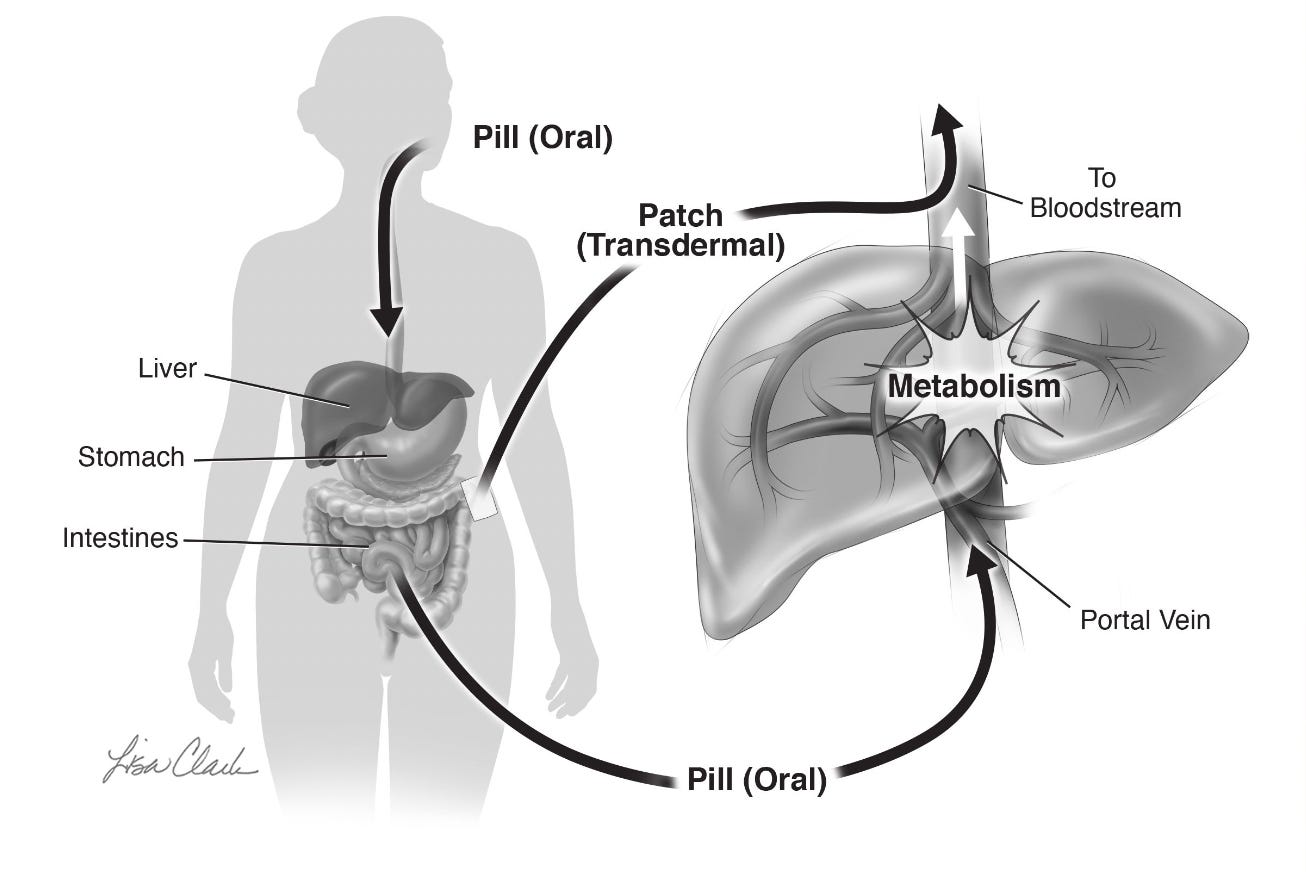
The liver is exposed to hormones in two ways. The first is like any organ, from the blood that circulates throughout the body. Unlike other organs, the liver also receives blood that comes from the bowel via a large vein called the portal vein, which carries nutrients, vitamins, and medications from food. It transports them to the liver, where they are metabolized (sorted and packaged for use or removal from the body via the gallbladder). When estrogen and progestin/progesterone (or any medication for that matter) are taken by mouth, they travel via the portal vein to the liver. This is called the “first pass’ effect, and I like to think of it as the liver getting the first pass at the medications. As a result, the liver receives higher levels of hormones than any other organ. This is why oral estrogen has a bigger effect on blood clotting. The metabolism of some hormones that arrive via the “first pass” can also lead to inflammation, which can, in turn, have negative effects. This means transdermal estrogen is always the safest for the liver and that progesterone is likely safer than progestins because we believe it to be less inflammatory.
Here’s an illustration, by Lisa Clark, of the first-pass effect from my book The Menopause Manifesto.
What We Know