


Menopause is Having a Moment
But it's veering into over medicalization

If you are following the online “menopause space” you might be aware of a dust up related to an op-ed published in the British Medical Journal about normalizing menopause (you can read it here).
Before we get into it, I want to make a disclosure up front. The op-ed suggested a video about menopause that I made with TED as an evidence-based resource for people to learn about menopause (you can watch the video here). To get that kind of recognition from experts in the field is an honor. I didn’t see their recommendation until after I read through the op-ed and had already informed my opinion, but I want to let you know up front, because that’s how I roll. Also, in my day job I get paid the same whether I talk about exercise, eating a balanced diet, using hormones, or following non hormonal options.
The article’s thesis is that menopause is a normal life event experienced by half the population. It explains how symptoms vary by country and culture and that there has been a recent return to over medicalization, similar to what we saw in the 1960s. The last few years have seen a surge of doctors, books, and apparently even a documentary promoting incorrect information about menopausal hormone therapy (a.k.a hormone replacement therapy), such as it’s "essential for every woman, that it can help with weight loss, that it prevents dementia and heart disease, that it is safe for women with breast cancer, and that many more women should be on testosterone. Some of these people even call menopause a “hormone deficiency disease” or a state of “female hormone deficiency”, which as you will see shortly is literally Pharma messaging from 1966.
To counter this growing chorus of “menopause as a disease” the op ed challenged the notion that menopause signals “decay and decline”, explained how experiences vary widely around the world, and that medicalization prepares women to expect the worst. Here are the take away messages:

So you might think, what’s the problem with an op-ed that explains how symptoms can vary based on country and culture and how the medicalization of menopause can lead to over treatment? No one would argue with an article like that about pregnancy. If someone wrote an article explaining how pregnancy is normal, that there are many things you can do to have a healthy pregnancy, and that fear based messaging about pregnancy can lead to an increase in the c-section rate, but that some people might need a c-section, I think it would be applauded.
That was the BMJ op-ed, just about menopause. I found none of it shocking, but I am familiar with the literature. The fact that symptoms of menopause vary around the world is something I discuss because it’s something people should know.
What I did find shocking were the comments that followed the op-ed. Strawman after strawman. An op-ed that normalizes menopause experiences around the world and raises concern about Western over medicalization and calls for more education is apparently problematic…because of all the things that the article wasn’t about?
Apparently some people feel that an op-ed that suggests education about menopause is vital and that a holistic approach, considering all options is somehow sets women back? An op-ed that rightly points out that the experience of menopause is negatively affected when when youth and reproductive status are revered (hello patriarchy) is somehow regressive? And that pointing out the truth that in countries where menopause is viewed simply as a phase of life, women are less bothered by symptoms than in countries where the “disease model” triumphs is a very dangerous narrative?
You can have terrible hot flashes and menopause not be a disease, just like you can have terrible labor pains and pregnancy not be a disease. Or like you can have terrible acne at age 14 and puberty not be a disease.
This wasn’t an op-ed about pharmaceutical versus non-pharmaceutical options, it was simply a call to be aware that over-medicalization is not the solution for women feeling unprepared for menopause. And while it is true that many women do have their concerns dismissed, the answer to that issue is not to recommend menopausal hormone therapy for every woman, nor to prescribe hormones for indications not supported by the literature.
It’s important to set the stage for this op-ed. The concern about the chorus of misinformation and frankly disinformation about menopause recently compelled the British Menopause Society to put out a statement. I gather the call is coming from inside the house, otherwise I’m not sure why the British Menopause Society would be involved? The recent British Medical Society statement on best practices for menopause, which are also endorsed by the Royal College of Obstetricians and Gynecologists and the Society for Endocrinology, states:
Hormones aren’t indicated for reducing the risk of dementia.
Testosterone replacement can help some women with with low sexual desire, but it shouldn’t be offered to improve cognitive function, musculoskeletal health, bone density or to prevent fractures.
Advice given to women with a history of breast cancer should be in line with national and international guidance on this matter. HRT replacement in women with a history of breast cancer, regardless of receptor status, should be seen as an exception.
For those of us who have been in OB/GYN for over 30 years and who have spent a lot of time reading about the history of menopausal hormone therapy (there is a chapter devoted to that in The Menopause Manifesto) this feels like a case of what’s old is new again. Menopause became a disease in the 1960s because it was profitable to Pharma, and we are seeing that again today, just with bespoke menopause therapies. Look, it’s a tried and true business model.
Before the hormone boom of the 1960s, hormones were largely a messy affair, think powdered extracts from cow and hog ovaries that were absorbed poorly. It turns out that many hormones need chemical modification so they can be absorbed from the gut, which makes sense as we didn’t evolve to get them from our diet. There were also injections that produced hormone levels that swung wildly as technologies for depot injections, those that disperse slowly over time into the blood, didn’t yet exist. But by the 1940s technology emerged to mass produce pills that were absorbed well.
Enter the medical menopause.
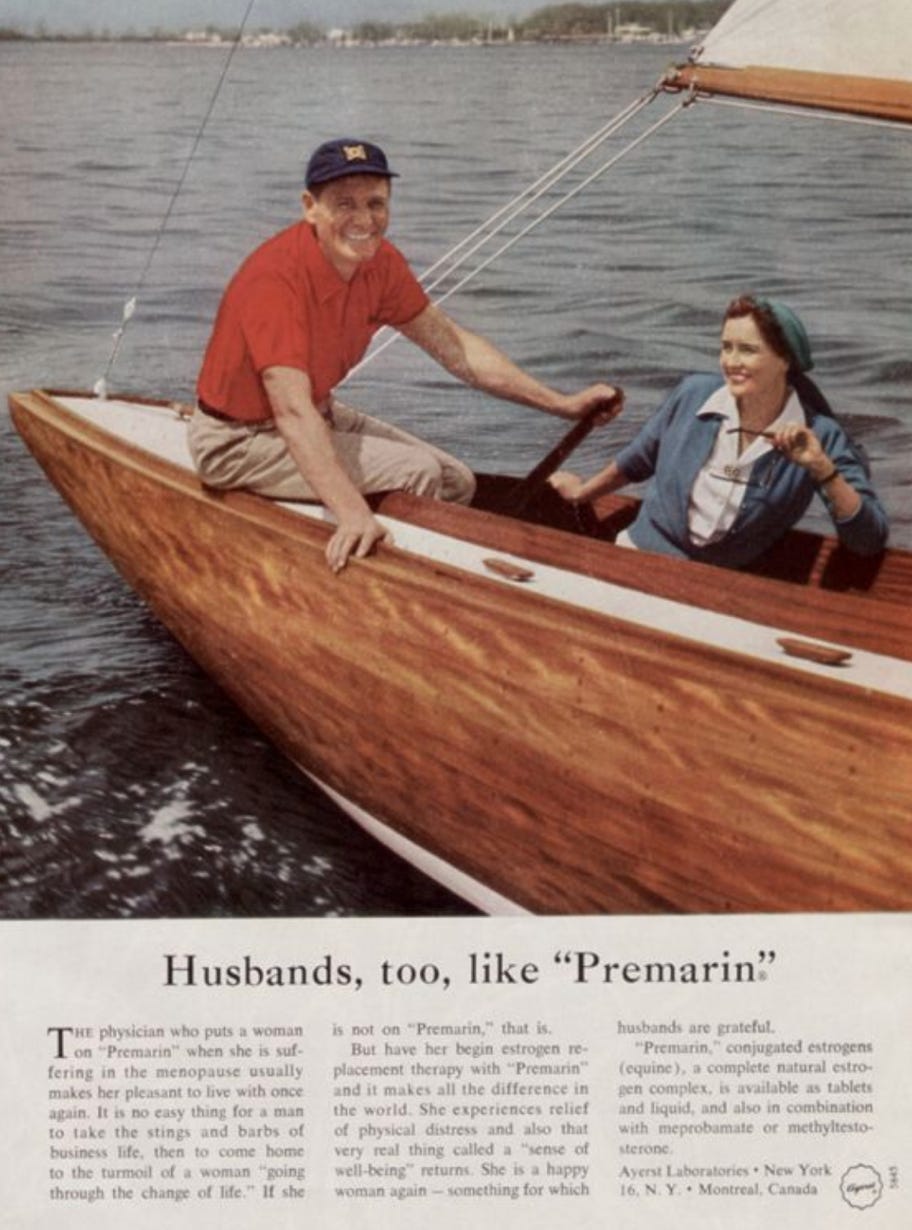
The ads were awful. Menopause was described as a disease, and not just any disease, the worst disease imaginable. ONE THAT MADE WOMEN HARPIES AND UNATTRACTIVE TO MEN.

Yes, even men liked Premarin! I guess it fixed their ugly-ass wives!
But the real catalyst for this hormone revolution wasn’t until the book Feminine Forever, written by Dr. Robert Wilson in 1966. It sold over 100,000 copies in the first year. The book falsely suggested women were never meant to live into menopause, hence it’s a disease (to any doctor who still thinks this, I beg of you, learn that average life expectancy does not tell us how long people lived and take a look in the mirror, because when you erase women after 50 you are the patriarchy). The answer to this dreaded modern disease of menopause was estrogen. It would keep you looking hot in tennis skirts (that tidbit is actually in the book). In the book I also learned that men judge a woman’s attractiveness from the ankle up. Not creepy at all.
But because no one else was talking about menopause in the 1960s, Feminine Forever not only became a bestseller. Its message also contaminated a lot of medicine. Of course later we found out that it was Pharma funded. And this is key, because when no one talks about menopause gaps can be exploited by people looking to profit.
The narrative of Feminine Forever is that menopause is “a hormone deficiency disease”…it’s literally on the cover. And yet here we are in 2022 and there are doctors using this same, incorrect, tagline! This incorrect deficiency narrative is becoming so pervasive that in their statement the British Menopause Society was very clear, “Menopause is a life stage and does not represent a deficiency state.”
A hormone deficiency implies that everyone with the condition needs treatment, for example a low thyroid or type 1 diabetes. This is not the case for menopause. Women have been outliving men since before modern pharmaceuticals. In fact, in 1966, the year Feminine Forever was published, the average life expectancy of a woman in the United States was 6-7 years longer than a man’s. Someone could have just as easily written a book that says men suffer from a menopause deficiency, because women outlive men!
And it’s not just me, or the British Society who say menopause isn’t a “female hormone deficiency.” No legitimate medical society or textbook refers to it as such.
What is gained by inaccurately positioning menopause as a disease? It scares people into the false narrative that everyone needs hormones. I hear from many women who have no symptoms who worry they should be on MHT because of what they read about their apparent “deficiency.”
My position is that we can and should educate about menopause, but scare tactics have no place. A false message is not helpful and, quite frankly, they aren’t needed. Women want more information, you don’t have to jazz it up. Also, women are intelligent, and when given facts instead of fear mongering, they make excellent decisions about how to manage their menopause if needed.
Menopause is having a moment, and that’s great. It is unacceptable that women enter this phase of life unprepared. And it is true that some women have distressing symptoms that need treatment. But it’s unacceptable to me that some people find the answer to the very real problems of being unprepared and the real problem of some being under treated, is to upsell hormones as an everywoman miracle cure.
The BMJ article was basically a call to remember our not so recent harmful medical past about menopause narratives and over medicalization, to educate about the world wide experience, and to combat stigma. Getting huffy about that is a weird flex. Either that or perhaps it was too on point?
So with so much misinformation and disinformation online, what is someone who wants to know more about menopause to do?
I encourage people to look to the legitimate medical professional societies, like the North American Menopause Society, the British Menopause Society, the Australasian Menopause Society and the National Institute for Health and Care Excellence (NICE). They are all pretty much in agreement and their guidelines are available online. Just Google the subject and add the name of the society. For example “testosterone menopause British Menopause Society”.
Get two sources. So if your doctor says something about menopause, you should also be able to find it from one of these societies or perhaps even in my book The Menopause Manifesto.
Ask yourself, if a few doctors don’t follow these guidelines because they have “cutting edge knowledge” (whatever that is) or feel they can better interpret the studies, what does that say? That this minority have truly found something that the vast majority of world experts missed when writing these guidelines? Or perhaps, just perhaps, this minority is incorrect? Those are the only two answers I can think of.
There are many options for symptom management, some hormonal and some that are not. Here are the evidence based takeaways:
Menopausal hormone therapy or MHT, meaning estrogen (with or without a progestogen, depending on if you have a uterus or not), can help with hot flashes, night sweats that disturb sleep, vaginal dryness and prevention of bladder infections, low mood in the menopause transition (not actual depression) and low libido.
MHT is not indicated for prevention of dementia or prevention of cardiovascular disease.
MHT is not recommended for people with a history of breast cancer.
MHT can also help prevent osteoporosis if you are at risk, but not everyone is at increased risk. You can use the FRAX tool here to calculate your risk. Click under the calculation tool.
There are also non hormonal options for hot flashes, night sweats, prevention of osteoporosis, and low libido.
We need more conversations about menopause. People deserve to know what is happening to their bodies and when they are suffering they deserve help, but a disease narrative is not the answer. It’s a patriarchal Feminine Forever callback and I’m not here for it. Women deserve facts, not a recycled patriarchal Pharma tagline.
It's a total mess. Noone can agree what women who have symptoms should do.
One can try to subjectively evaluate how "bad" one's symptoms are I guess, and that's what I have heard from doctors, but I'm not sure we are really good at that type of evaluation, of how much we should put up with as annoyance (regular hot flashes that aren't severe say but that are annoying), how much we should grin and bear, and what we should treat. And then there is the question of how best we should treat it. And patients aren't in the best position to know that either.
I tend to think pain and discomfort should be treated, I won't say how, that is for doctors and scientists! And I genuinely wish we had better treatments than we do, I hope some day we do. But often the belief with menopause is that it's a pain that shouldn't be treated, because some treatments have some risks or downsides, or because menopause "is natural". Or that if somehow we lived in a different country, a different culture etc., our symptoms would be less. So therefore even though we can't move to an entirely new country for symptom relief, it's not remotely realistic, symptoms shouldn't be treated.
I think it's kind of inevitable if one doesn't treat with pharmaceuticals one will keep *trying* to treat with vitamins and herbs and so on. Because the innate desire to feel better is still there, it's just being human, even if one convinces oneself the hardships are bearable (and maybe one's hardships are more minor that say one's menopausal friends symptoms, and thus in some sense more bearable, and I don't see any way to even quantify the difficulty except relatively). Most of the vitamins and herbs are harmless of course, so this isn't causing harm. But as you say there isn't much data they work!
I don't think women with no symptoms need to all rush out and get an MHT prescription, but I wonder how many people that really describes (25% of women going through menopause max maybe?). I mean mostly the choice is live with symptoms or try to treat symptoms in some way. That's the choice. Not whether or not to take MHT for no reason.