


Eight Takeaways from the 2024 Menopause Society Meeting
Hair loss, diet, brain health and more


The 2024 Menopause Society meeting in Chicago has come to a close. I really enjoyed the content; I learned some new things and had my conclusions about several topics supported. For example, I was thrilled to see that my post on hormone therapy and dementia (this one here) was exactly in line with Dr. Maki’s talk on the state of the literature on hormone therapy and cognition and dementia. I will write a post about her talk because it was that good. She is a world expert and is doing great research. (Note: Dr. Maki leads NIH-funded research focused on the role of hormones on cognition, mood, and brain function).
Something very interesting happened at the meeting outside of the lectures: 50 or 60 health professionals came up to me to discuss the menopause misinformation their patients are getting from medical professionals, coaches, and celebrities on social media and podcasts. I was thanked by so many for supplying an evidence-based, reliable source. I heard stories of women advised to lie about having low libido to get testosterone, asking for excessive doses not recommended by the guidelines, and turning down statins because they believed hormone therapy was the unique key to preventing heart disease.
This sadly doesn’t surprise me, and I even wrote about the rise of menopause misinformation in a previous post. If doctors with hundreds of thousands or even millions of Instagram followers are posting content that says hormone therapy prevents dementia, which is not at all supported by the latest evidence, it’s not surprising people come in misinformed. Most people only get 15-20 minutes with their health care professional, and when most of that time is spent undoing the misinformation the patient learned online, that is a lot of lost time that could have been used for discussing evidence-based care. While sometimes the patient walks away properly informed, many times it’s impossible to correct in 20 minutes what the patient has heard for hours from various sources, most of whom have created a self-referential echo chamber of misinformation designed for their own profitability.
It was notable that last year at the meeting (2023), I heard about this misinformation from just one of two providers, but this year, it was a steady stream of people every day of the meeting. It’s clear I am not the only one who has noticed the increase in misinformation in the past year. It’s sad because there are enough valid reasons to prescribe hormone therapy, but I guess sticking to facts doesn’t get as many page views because the algorithm favors fear. Perhaps it’s hard to charge $1,500-$3,000 for an hour's visit to provide the same recommendations as found in guidelines available for free.
Here, I want to give you eight quick takeaways from the lectures. Keep in mind that these are not full reviews of the subject but information from the speakers.
Hair loss #1. If your hair loss issue is that your hairline is receding, you need to see a dermatologist. You must be evaluated for frontal fibrosing alopecia, a type of hair loss that involves scaring, as the hair can’t grow back if left untreated. It is often unmasked during the menopause transition or during menopause but can affect people of all ages and genders. For some unknown reason, the incidence is increasing. There are treatments to stop the progression, so if you are concerned your hairline is receding, then please see a dermatologist.
Hair loss #2. The most common type of hair loss during menopause is female pattern hair loss. It typically presents as a thinning part line and/or a thinning ponytail. Hair typically goes through three phases: anagen (growing), catagen (stops growing, starts to detach), and telogen (the hair follicle rests and there is no growth). With female pattern hair loss, more hair enters telogen, so more is lost, and then when the hair follicle wakes back up to start anagen again, the hair follicle has become miniaturized, so the hair is finer and doesn’t grow as long. It’s important to rule out other causes of hair loss, such as low iron or taking testosterone. When the diagnosis is certain, the first line therapy is either oral or topical minoxidil, and while they are equally effective, topical minoxidil must be used twice a day, and many people can’t do that or don’t like it (which I totally understand). Oral spironolactone can also be added. There was no mention of supplements, and FYI, there is no data to support biotin. The speaker’s go-to starting regimen is oral minoxidil 1.25 mg and spironolactone 100 mg.
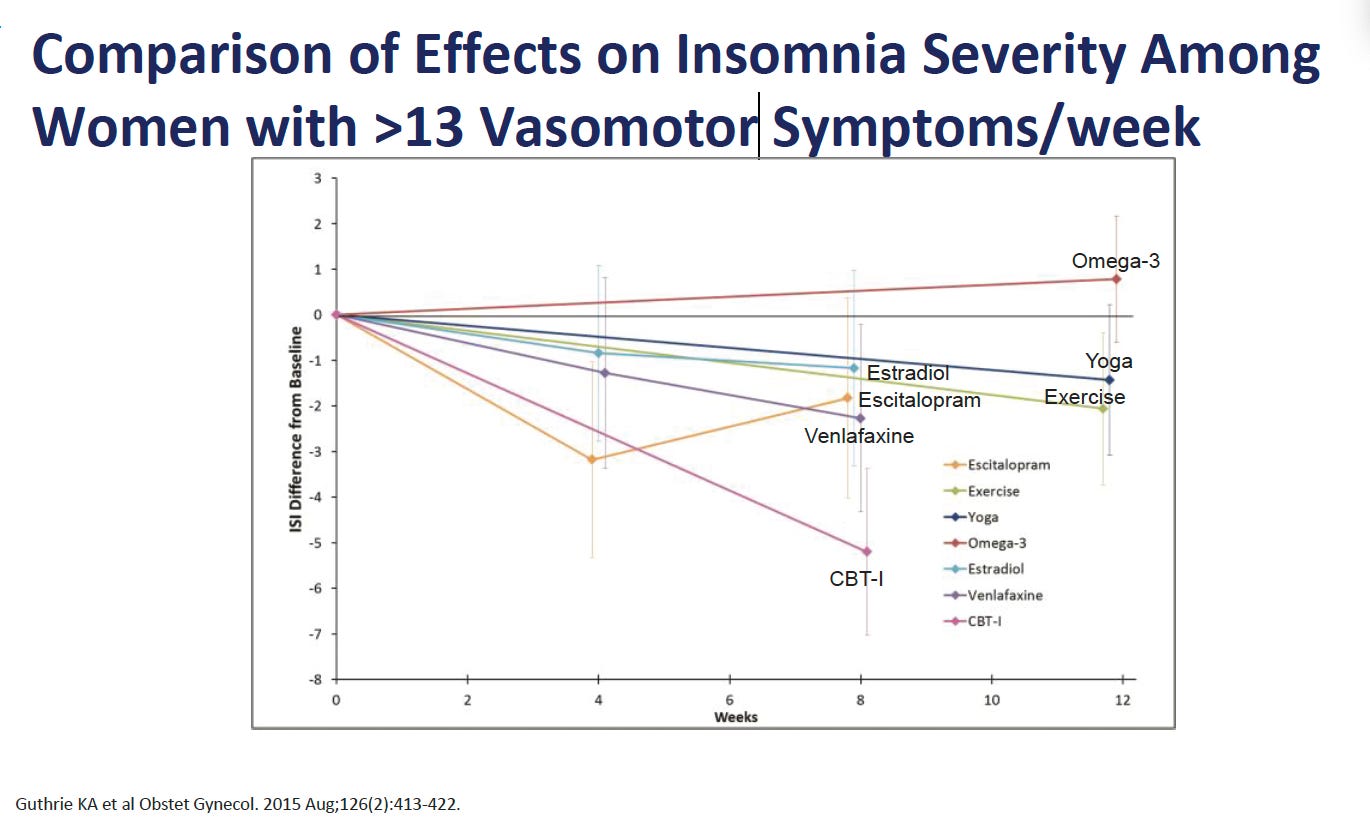
Sleep #1. Cognitive behavioral therapy for insomnia, or CBT-I, is the most effective therapy, even when there are hot flashes! CBT even outperformed estrogen (although in the study presented, the estrogen was admittedly a lower dose, 0.5 mg oral estradiol). The take-home message here is that CBT-I works whether there are hot flashes or not, and a review of the literature was presented that suggests that menopause hormone therapy only has a modest improvement in sleep quality. Many women have poor sleep, even when hot flashes are improved with therapy, so consider CBT-I as a good add-on or complement to pharmaceutical therapies, and it is also a totally reasonable thing to do as a stand-alone. Pro tip: keep this in mind if you have started a moderate dose of estradiol (a 50 mcg patch or 1 mg oral) and are still not sleeping well. Unless you are waking up soaked in sweat multiple times, maybe consider CBT-I as an add-on. I think it’s important to see this slide, which shows that many of the nonhormonal therapies are also good for sleep in menopause for people who have hot flashes. Even more interesting, the CBT-I therapy in this study, as shown in the image below, was delivered by telephone.
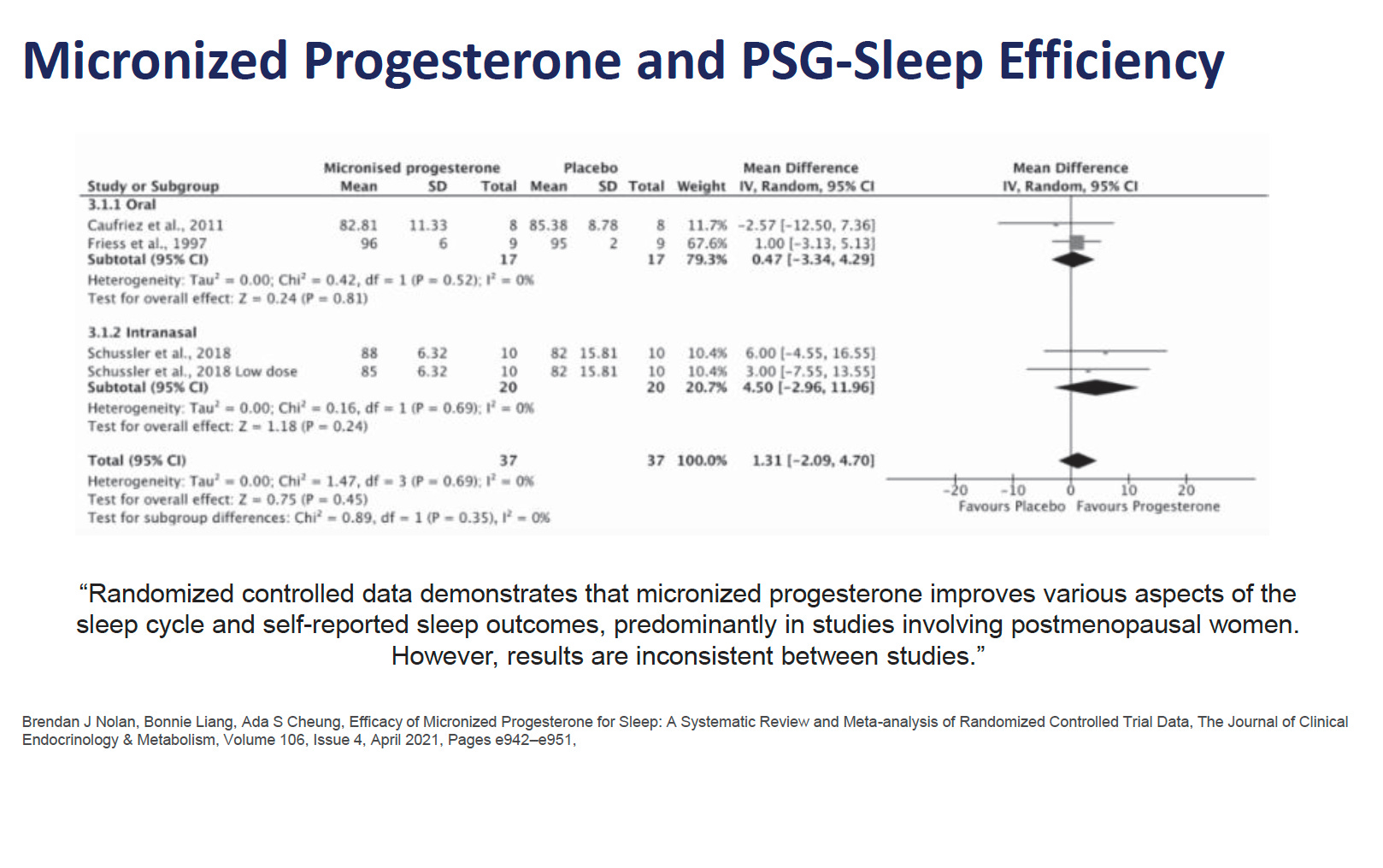
Sleep #2. Progesterone may not be as effective as we think. Many of us have heard that progesterone is sedating and can help with sleep. However, there is a massive placebo response in sleep studies, so that is always important to keep in mind. This is the slide from a recent meta-analysis that was presented. I’m not saying people should stop their progesterone if they are sleeping well, but if it’s not working, maybe consider that it doesn’t have the most robust evidence, and the reason you are still not sleeping well might be because you may not be taking an effective therapy.
Diet. The takeaway was that the best diet is likely a Mediterranean diet focusing on lean and more plant-based proteins. No surprise. The lecturer didn’t even mention intermittent fasting, but it came up in the questions. No surprise there either, as there are two books from providers with massive followings on social media that make some pretty bold (and scientifically unverified) claims about intermittent fasting being superior for women. The speaker, Annina Burns, PhD, RD from the Office of Research on Women’s Health at the National Institutes of Health (NIH), said that if you were to design the worst diet for perimenopause, it would be intermittent fasting. The speaker felt that the impacts of hormonal fluctuation in the perimenopause of inflammation could be worsened by time-restricted eating and, in fact, thought scientifically the best diet in perimenopause was more likely to frequent small meals, although admittedly not studied. Look, if intermittent fasting works for you, great, but anyone who is suggesting it is especially beneficial for perimenopause has it wrong.
Impact of vasomotor symptoms (hot flashes and night sweats) on health outcomes. People with more VMS seem to be at higher risk for cardiovascular disease (CVD) and dementia. This doesn’t mean that you will definitely get CVD or dementia if you are a super flasher, nor does it mean that treatment of hot flashes/night sweats will prevent these outcomes. While one hypothesis is that hot flashes are involved in a causal relationship with CVD and/or dementia, it’s equally plausible that VMS is a marker. For example, it’s possible that people who are destined to get CVD or dementia have more blood vessel stiffness, and the stiffness is also what makes them more likely to get hot flashes. And there are many other explanations for a correlation between the two instead of a cause and effect. This is an active and important area of research. The take-home is that we don’t want women to suffer, so it’s important to treat hot flashes, and hopefully, over time, we will learn if that treatment also reduces the risk for CVD and dementia for the subgroup with more hot flashes.
The voice. Testosterone can lower the voice, even when dosed appropriately, and this is a real risk. While understudied, blood levels can’t predict this. If you use your voice professionally, this should be a consideration, although it should be a consideration for everyone as the changes are largely irreversible.
Cognitive behavioral therapy (CBT) and hot flashes. There is good evidence to support using CBT for hot flashes. This does not mean that everyone needs to try it; it is just one more option as a stand-alone therapy or as an add-on to other therapies. Thoughts and mood affect our physical experience; of course, the reverse is true. I think we can all understand that controlling that response may be beneficial if we feel sad or anxious, embarrassed or angry because of a hot flash. CBT can help with cognitive distortions that might negatively amplify the hot flash experience. This doesn’t mean the hot flash is made up or in your head; it just recognizes that there is a mind-body connection, and it can be a powerful tool you can use to your advantage. Also, CBT for hot flashes also focuses on the concept that any improvement is good. I think many of us, myself included, look at therapies in an all or none way, but the reality is many therapies improve things by 50% or 60%, and sometimes cognitive distortions may keep us from appreciating and enjoying that improvement. Side note: I see some healthcare professionals with large accounts disparaging CBT for hot flashes. That tells me they have not bothered to read any of the literature or somehow offering nonhormonal therapies interferes with their bottom line. I simply can't imagine a situation where I would shit on an evidence-based therapy that is safe. More science-backed options are good for women. That is the hill I will die on.
That’s my summary from 28 pages of notes. If this format interests you, I may write some more quick takeaways. Stay tuned for a longer post on the lecture on cognition and dementia!
This is summary of the menopause conference is super helpful and detailed! I look forward to your future post about Dr. Maki's presentation on dementia, hormone therapy and cognition.
I love that CBT has shown so many positive effects for menopausal women. Women are being pulled in so many directions these days--work, partner, kids, to be the perfect size, home maker, etc. Having someone to talk to and work through things is incredibly helpful. Movements, diet, therapy are all massive game changers.