Starting MHT is a big topic because there are quite a few choices. And while choices are great, the permutations and combinations can sometimes leave people with decision paralysis. It's like the Cheesecake Factory with its impossibly long menu. How does one decide? Can’t there be a MHT prix fixe?
Here, I am going to discuss the estrogen in menopausal hormone therapy (MHT). It is estrogen that provides the benefit for most (if not all) of the symptoms. Specifically, we’ll cover what steps and tests you should take before getting started (including calculating breast cancer risk) and the different types of estrogen. The following posts in the series will address the progesterone/progestin (also known collectively as progestogens) part of the hormone equation, which is only necessary if you have a uterus. And then we’ll get to doses.
We will not be discussing compounded hormones or pellets, which are a waste of money and potentially dangerous. You can read more about that here and why the terms “bioidentical” and “body identical” are meaningless. I could give someone massive doses of estradiol extracted from human ovaries and, in a few short years, give them endometrial cancer. Meaning I could prescribe a 100% genuinely bioidentical and natural therapy that also happens to be 100% unsafe. So try to ignore terms like “bioidentical” and “body identical” because they are marketing terms.
Before we begin, short-term use of appropriately dosed MHT, meaning less than five years, is incredibly safe, assuming you don’t have significant contraindications to menopausal hormone therapy (which I have covered in several posts here (age of starting), here (cardiovascular disease) and here (liver disease). This doesn’t mean longer-term use is unsafe; we just have less long-term data. When starting, I suggest setting aside the long term and focusing on the short term because immediate needs, like hot flashes and night sweats, depression, or joint pain, are almost certainly why you are starting the medication. It can be overwhelming to try to decide about medication for 10 or 15 years when:
You don’t know how you will feel on the therapy
The late menopause transition and the first year or so of menopause are often the worst times for symptoms, so once you are over that hump you may not need estrogen long-term
You can change because you haven’t made an unbreakable vow with your hormone choice
You may feel desperate for relief, and once you feel better, it might be easier to think about the longer-term
Over time, we may get new information about hormones, or you may get new information about your health, which could clarify or change things for you
Questions and Tests to Get Started
The risks of menopausal hormone therapy primarily revolve around risks to the cardiovascular system, blood clots, and hormone-sensitive cancers (most commonly breast and endometrial), so some questions and tests can help us determine safety.
Here are six steps to take before starting MHT:
Review your medical history. If you have previously had breast cancer, then hormones are not recommended. Hormones may be considered for some who have had early-stage, low-grade endometrial cancer, but that is something that can only be decided with your own providers who know your history. Also, liver disease is a case-by-case discussion, as discussed here, and recommendations about hormones for those at higher risk for blood clots range from not recommended to maybe okay for some.
Report any irregular bleeding or bleeding after your last period to your provider. Any bleeding AFTER your last period must be investigated before starting hormones. Irregular bleeding before menopause may be entirely typical and not concerning, or it could be concerning. Make sure your provider knows so they can decide, based on your bleeding pattern, medical history, and family history, if this is just regular but bothersome menopause transition bleeding or if any other testing to rule out precancer or cancer of the lining of the uterus is needed before starting hormones. Your bleeding may not need any testing, but only your provider, who knows you, can make that call.
Get a mammogram. One, we want to ensure someone doesn’t have breast cancer before giving them hormones. The other reason is to know breast density, which can be used to calculate breast cancer risk. People with dense breasts have double the risk of breast cancer, and knowing this might inform some of the decisions around hormone therapy, especially for people with extremely dense breasts.
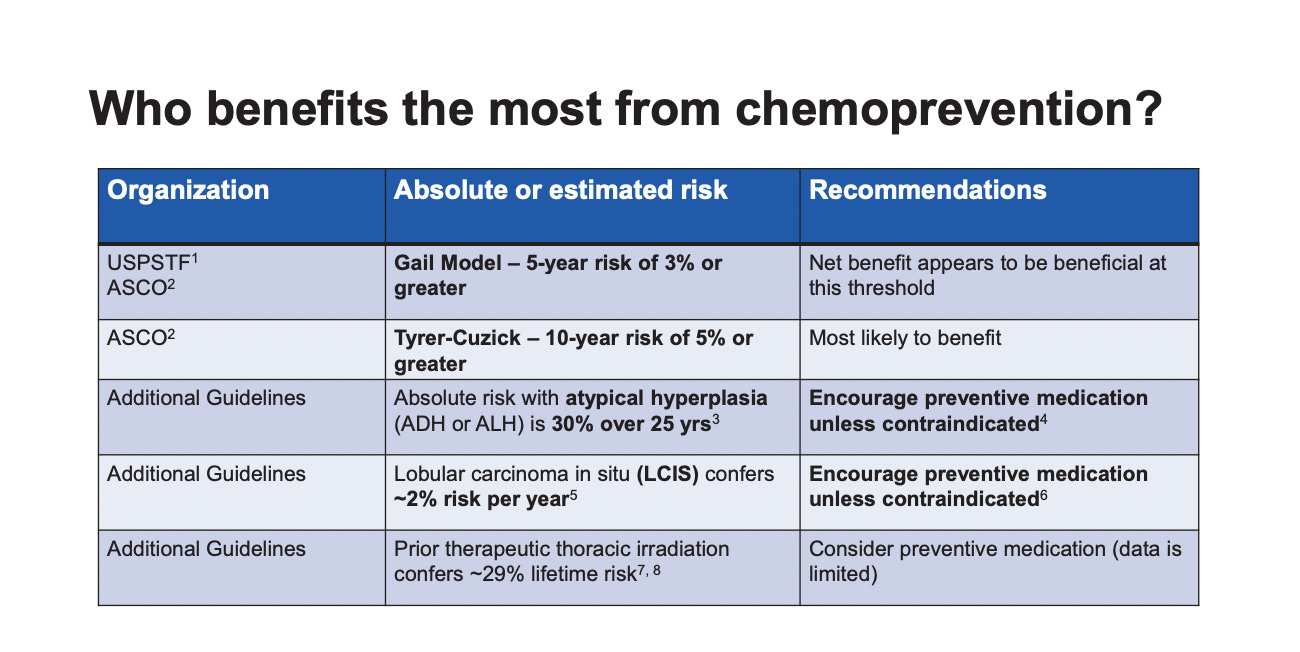
Calculate your breast cancer risk. Two relatively easy tools are the Gail model (no mammogram needed) and the BCSC Risk Calculator (mammogram needed). If the risk of breast cancer in the next five years is 3% or greater or 5% or greater in the next 10 years, then guidelines recommend offering medications to reduce the risk of breast cancer. In fact, guidelines recommend discussing risk-reducing medications for anyone with a 5-year risk of > 1.7 by the Gail model. Here is a slide from the Menopause Society meeting breast course (September 2023) showing who is likely to benefit the most from medications to reduce the risk of breast cancer.
The Endocrine Society has more defined recommendations about MHT regarding breast cancer risk than other societies. Per their guidelines, if your risk for breast cancer is high enough to recommend a risk-reducing medication, it’s probably wise to get more information about your breast cancer risk and these medications before starting estrogen.
Here is the Risk Cutoff table from the Endocrine Society:
Calculate cardiac risks. Know your blood pressure, have a lipid profile, and get screened for diabetes. This information is needed to calculate ASCVD, the risk of a major cardiovascular event in the next 10 years. Read more about cardiac risks here.
Know your risk of osteoporosis. The OST or FRAX are two different tools. If you are at higher risk for osteoporosis, that might influence your decision to start hormones. For example, if you have joint pain, estrogen may or may not help, but if you are also at high risk for osteoporosis, you might be more inclined to try estrogen. Also, knowing your OST or FRAX can help you advocate for a bone density scan if you are at higher risk.
The Estrogens
Your next step is to consult with your physician about the choice of estrogen. There are two main options for standard MHT.
One is estradiol, which is as close to identical as possible to the estradiol made by the ovaries (but not “bioidentical” because no estrogen made in a lab can truly be identical to what the ovary makes). Estradiol is the main estrogen made by the follicles. The other choice is conjugated equine estrogens, or CEE, known as Premarin. CEE is extracted unchanged from pregnant mares' urine. CEE is a natural estrogen, and all estradiol is made in a lab. But natural or lab-made, or similar to what the ovaries make or not, has nothing to do with safety. Studies are what inform us about safety. It’s a good idea to ignore the marketing terms and simply learn about estradiol and CEE. When someone advertises that they specialize in “bioidentical hormones,” I just roll my eyes. If we’re going to use those terms, then all estradiol is “bioidentical,” and there are plenty of safe government-regulated options. Also, all estradiol that is made in a lab is made from a chemical found in soy or yams.
There is a third option that we will discuss in another post, which is estrogen-containing contraception. This is only used for people before menopause when they need contraception and/or control of their menstrual cycle. Standard MHT can be used during the menopause transition or in menopause. Here, we will confine ourselves to standard MHT.
There are two main areas of risk to consider when selecting the type of estrogen:
Heart health/blood clot risk: Transdermal estradiol is the safest. If your ASCVD is 5-10%, then you should only consider transdermal, and if it is > 10%, then estrogen of any kind is not recommended. Only transdermal estradiol can be considered for people at higher risk for clots, and this requires shared decision-making. You can read more here.
Breast cancer risk: Premarin (conjugated equine estrogens) is the lowest risk and even lowers the risk of breast cancer over long-term risk. At the recent Menopause Society meeting (September 2023), one of the speakers mentioned that Premarin had more than 17 hormones, and the theory about the reduction in breast cancer risk is one or more of these hormones may act like an anti-estrogen on the breast. He did not think that a synthetic (lab-made) version of Premarin would be possible given its molecular complexity (as I know someone will want to know if there is a non-horse urine-derived option). While there is data that suggests estradiol is not associated with an increased risk of breast cancer, we don’t have a lot of clinical trial data here. However, if there is a risk with estradiol, it’s likely quite low. It is essential to keep in mind that estrogen increases breast density, which can affect mammogram quality. For those with a uterus, the progestogen therapy needed to protect the uterus is believed to contribute more to the breast cancer risk than estradiol and can negate the beneficial effects of Premarin. We’ll discuss this in the next post.
Putting it Together
Someone at low risk for heart disease (ASCVD < 5%), low risk of clots, and 5-year breast cancer risk < 1.67%, who is within 10 years of their last period or less than age 60 and has no other reason where hormones are contraindicated can really pick whatever estrogen therapy appeals to them, but as transdermal estradiol is believed to be the safest from a clot perspective, that is the recommended starting therapy. For someone in this low-risk category, trying MHT for non-FDA-approved reasons, for example, depression, joint pain, or burning mouth, is something I’m very comfortable with because six months of transdermal estradiol to see if these types of symptoms improve is about as low risk as it can be for a medication.
For someone with an ASCVD risk of 5-10%, transdermal estradiol is recommended. With a higher risk category, it’s a longer discussion about benefits vs. risks, especially for non-FDA-approved indications. There is a lot of shared decision-making here, and only your provider, who knows your symptoms and medical history, can help. The greater the risk, the more we want to stick with the FDA-approved indications. It’s always important to remember that we have non-hormonal medications for hot flashes and night sweats, which is also an important part of the discussion.
For someone at higher risk for clots, the decision to use transdermal estradiol therapy needs to be individualized and likely only considered for severe hot flashes or night sweats when other options have failed and in conjunction with a hematologist. When this question came up at the Menopause Society meeting, there was lots of hemming and hawing about who might be an okay candidate for hormone therapy. I know there are some people who are cavalier about giving transdermal estrogen here, but the Endocrine Society and Menopause Society guidelines don’t support hormone therapy for people at higher risk of blood clots. The Australasian Menopause Society states, “More research is needed prior to advocating the use of a patch in women at high risk of DVT,” and the British Menopause Society states, “Discussion with a haematologist should be considered in postmenopausal women at particularly high risk.”
More discussion about estrogen choice is needed for someone with a higher risk of breast cancer (5-year cancer risk > 1.67% and definitely > a 5-year risk of > 3%). Premarin may be a consideration for some people, given its association with a lowered risk of breast cancer. This will take shared decision-making with your provider. When breast cancer risk is increased, a consultation with an expert in breast cancer prevention before proceeding is generally a good idea, especially for those with 5-year risks over 3%. It is important to have all the information to make an informed decision.
For people with a uterus, Duavee, which is Premarin plus bazedoxifene, gives you the benefit of Premarin (you can read more about it in this post). Some data shows that Duavee is associated with a reduction in breast density, so that might also be a consideration for someone with extremely dense breasts (you need the bazedoxifene part to get the reduction in breast density).
Summary
The prix-fixe menu for MHT is transdermal estradiol, but the alternative menu might be Premarin or Duavee.
For those who dislike transdermal therapy, oral estradiol isn’t wrong for someone at low risk for cardiac issues or clots. Still, those issues increase with age, and for someone who thinks they want to stay on estrogen long-term, transdermal is likely the safer option.
Knowing your ASCVD and breast cancer risk scores before seeing your provider can help make the appointment easier.
For someone with an intermediate risk of breast cancer and an ASCVD risk of 5-10%, there will be some complex discussions and a lot of shared-decision making. Remember, we also have non-hormonal options for hot flashes, night sweats, and osteoporosis. so there are other options besides estrogen.
In the next post, we will get to the progestogens!
***
As always, the information here is not direct medical advice. If you have questions, leave them below. I try to reply to the easier ones directly in the comments (obviously, again, not individual medical advice). For those questions that are more complex, I tuck them away to try to incorporate them in future posts.
Santen RJ, et. al. Underlying Breast Cancer Risk and Menopausal. J Clin Endocrinol Metab 2020;105: e2299–e2307.
US Preventive Services Task Force. Medication Use to Reduce Risk of Breast Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2019;322(9):857–867. doi:10.1001/jama.2019.11885
Cynthia A. Stuenkel et. al. Treatment of Symptoms of the Menopause: An Endocrine Society Clinical Practice Guideline, The Journal of Clinical Endocrinology & Metabolism, Volume 100, Issue 11, 1 November 2015, Pages 3975–4011, https://doi.org/10.1210/jc.2015-2236.
The 2022 hormone therapy position statement of The North American Menopause Society. Menopause 2022;29:767-794.
Collaborative Group on Hormonal Factors in Breast Cancer. Type and timing of menopausal hormone therapy and breast cancer risk: individual participant meta-analysis of the worldwide epidemiological evidence. Lancet 2019; 394: 1159–68.
Fournier A, et. al. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat 2008;107:103–111.
Chlebowski RT, et al. Association of Menopausal Hormone Therapy With Breast Cancer Incidence and Mortality During Long-term Follow-up of the Women’s Health Initiative Randomized Clinical Trials. JAMA 2020;324:369–380.
Fabian CJ, et. al. Effect of Bazedoxifene and Conjugated Estrogen (Duavee) on Breast Cancer Risk Biomarkers in High-Risk Women: A Pilot Study. Cancer Prev Res (Phila). 2019;12:711-720. doi: 10.1158/1940-6207.CAPR-19-0315.
I can’t thank you enough for your clear, easy to understand information. You really cut through the clutter. I’ve been on Duavee for just over a month and have been a bit nervous about it as I haven’t been able to find much literature on it. I was prescribed it through the menopause clinic in Toronto and did ask questions about it. They were reassuring but I was still uncertain. Your article helped. You are my go to for all things menopause. I read the Menopause Manifesto and it was a lifesaver. I recommend it and your blog to all my friends!






I can’t thank you enough for your clear, easy to understand information. You really cut through the clutter. I’ve been on Duavee for just over a month and have been a bit nervous about it as I haven’t been able to find much literature on it. I was prescribed it through the menopause clinic in Toronto and did ask questions about it. They were reassuring but I was still uncertain. Your article helped. You are my go to for all things menopause. I read the Menopause Manifesto and it was a lifesaver. I recommend it and your blog to all my friends!
Once again - clear, concise info. - thanks so much.
Is MHT completely out of the question for over 70 - still have hot flashes and at risk for osteoporosis, but no other. issues?
I did have a 5 year stint or MHT at the beginning of menopause, but my doctor cited the studies regarding continued use and stopped it.